International Journal of Gynecology and Obstetrics (2008) 100, 4–9
a v a i l a b l e a t w w w. s c i e n c e d i r e c t . c o m
w w w. e l s e v i e r. c o m / l o c a t e / i j g o
A systematic review of randomized controlled trials toreduce hemorrhage during myomectomy foruterine fibroids ☆
E.J. Kongnyuy a,⁎, N. van den Broek a, C.S. Wiysonge b
a Child and Reproductive Health Group, Liverpool School of Tropical Medicine, Liverpool, UK
b South African Cochrane Centre, South African Medical Research Council, Cape Town, South Africa
Received 8 May 2007; accepted 13 May 2007
Objective: To assess the effectiveness and safety of interventions to reduce blood loss during
myomectomy. Methods: Electronic searches of the Cochrane Library, MEDLINE, and EMBASE,
between 1966 and 2006 for randomized controlled trials (RCTs). Results: We found significant
reductions in blood loss with vaginal misoprostol (weighted mean difference [WMD] −149.00 mL,
95% confidence interval [CI] −229.24 to −68.76); intramyometrial vasopressin and analogues
(WMD −298.72 mL, 95% CI −593.10 to −4.34); intramyometrial bupivacaine plus epinephrine(WMD −68.60 mL, 95% CI −93.69 to −43.51); and pericervical tourniquet (WMD −1870.00 mL, 95%CI −2547.16 to −1192.84). There was no evidence of effect in blood loss with myoma enucleationby morcellation and oxytocin. Conclusion: There is limited evidence from a few RCTs that someinterventions may reduce bleeding during myomectomy. There is need for adequately poweredRCTs to shed more light on the effectiveness, safety, and cost of different interventions to reduceblood loss during myomectomy. 2007 International Federation of Gynecology and Obstetrics. Published by Elsevier Ireland Ltd. All rights reserved.
☆ This paper is based on a Cochrane Review published in The
The standard treatment of symptomatic leiomyomas (myo-
mas or fibroids) is hysterectomy for women who have
information). Cochrane Reviews are regularly updated as new
completed childbearing and myomectomy for women who
evidence emerges and in response to feedback, and The Cochrane
wish to preserve fertility. Myomectomy can be accomplished
Library should be consulted for the most recent version of the
by laparotomy, laparoscopy, or hysteroscopy. Massive blood
loss associated with the dissection of huge fibroids renders
⁎ Corresponding author. Liverpool School of Tropical Medicine, L3
5QA, Liverpool, UK. Tel.: +44 151 705 3705; fax: +44 151 705 3329.
myomectomy a more technically challenging procedure than
hysterectomy. A requirement for transfusion in up to 20% of
0020-7292/$ - see front matter 2007 International Federation of Gynecology and Obstetrics. Published by Elsevier Ireland Ltd. All rights reserved.
A systematic review of randomized controlled trials
cases following abdominal myomectomy has been reported
omy (laparotomy, laparoscopy, or hysteroscopy) for uterine
in the literature, and in 2% of cases there is need for
fibroids for any reason. Only interventions performed during
conversion of myomectomy to hysterectomy
surgery, immediately before surgery, or within 24 h prior to
A number of interventions have been introduced to
surgery were considered for this review.
reduce bleeding during myomectomy. Three categories of
The primary outcome measures were estimated blood loss in
interventions can be identified: (a) interventions on uterine
milliliters and need for blood transfusion. Secondary outcomes
arteries such as laparoscopic uterine artery dissection,
included duration of operation, intraoperative hysterectomy,
uterine artery embolization, pericervical mechanical tourni-
conversions from laparoscopy to laparotomy, other intraopera-
quet and hormonal tourniquets such as vasopressin and
tive complications, duration of hospital stay in days, post-
terlipressin; (b) uterotonics such as ergometrine, oxytocin,
operative morbidity, post-operative hemoglobin and hematocrit,
misoprostol, and sulprostone; and (c) myoma dissection
abdominal revisions for hemoperitoneum or pelvic hematoma,
techniques which include the use of laser and chemical
post-operative recurrence of myomas, pregnancy (if pregnancy
dissectors such as sodium-2-mercaptoethanesulfonate
desired), treatment adherence, adverse events and cost (total
cost, and cost of the intervention).
Despite these procedures excessive hemorrhage during
myomectomy remains a major challenge to gynecologic
surgeons The effects of these procedures on blood lossduring myomectomy, as reported by previous non-rando-
Data were analyzed using RevMan 4.2 according to standard
mized studies, have been inconsistent . Moreover, the
Cochrane guidelines ; analyzing trial participants in groups to
types of these interventions are so varied that there is need
which they were randomized, regardless of whether they
to identify those procedures that are most effective and have
actually received the treatment assigned. For dichotomous
the least adverse effects to help the gynecologic surgeon to
data, we expressed study results as odds ratios (OR) with 95%
confidence intervals (CI). We were not able to assess for
The aim of this review was to assess, using the best
heterogeneity because of insufficient number of trials in the 7
available evidence, the effectiveness and safety of interven-
comparisons (intervention vs placebo/no treatment) considered
tions to reduce blood loss during myomectomy for uterine
in this review. Planned subgroup analyses based on the
fibroids. The use of pre-operative gonadotrophin releasing
technique of myomectomy (laparotomy, laparoscopy, or hys-
hormone (GnRH) analogues was not considered in this review
teroscopy), type of comparison group (placebo or no treatment),
because their effectiveness has previously been examined in
and ethnic background (black or white) were not performed for
For continuous data, we recorded the means and their stand-
ard deviations for each arm of the trial and expressed studyresults as weighted mean differences (WMD) with 95% CI. Where
only the median was reported, we assumed that the mean wasequal to the median (after checking for skewness) and estimated
Electronic searches were conducted in the Cochrane Menstrual
the standard deviation from the range (range × 0.95/4). Only one
Disorders and Subfertilty Group specialized register, Cochrane
comparison, hormonal tourniquet vs placebo or no treatment,
Central Register of Controlled Trials (Cochrane Library Issue 1,
had two trials. There was significant statistical heterogeneity
2006), MEDLINE (1966 to March 2006), EMBASE (1980 to March
between the study results (P b 0.00001, I2 = 98.8%). Thus, we used
2006), Current Contents (1993 to March 2006), the National
the random effects method to pool the data and investigated the
Research Register, and the National Library of Medicine's Clinical
Trial Register (up to March 2006), by combining search terms forthe health condition (myoma⁎, fibroids, leiomyoma) and the
interventions (myomectomy OR laparotomy, laparoscop⁎, hys-teroscop⁎, uterotonic⁎, misoprostol, sulprostone, ergometrin⁎,
We identified 17 potentially eligible studies, from which we
tourniquet, vasopressin, terlipressin, uterine artery ligation,
excluded 4 because further investigation revealed that there was
uterine artery dissection, uterine artery emboli⁎, mesna,
no randomization , and 5 because the control group was
chemical dissection, laser dissection, uterine fibroid emboli⁎)
another active intervention rather than a placebo or no treat-
followed by standardized methodological filters for identifying
The remaining 8 randomized controlled trials with 371 parti-
In addition, the above searches were supplemented by
cipants met our inclusion criteria: two trials with 58 participants
contacting experts in the field of myomectomy (for unpublished
on a hormonal tourniquet, vasopressin ; one trial on the
data) and a hand search of specialist journals, conference
uterotonic effect of misoprostol one on oxytocin ; one
abstracts, relevant review articles, and reference lists of iden-
on pericervical tourniquet one on chemical dissection with
tified trials. There were no language restrictions to the search.
mesna ; one on the vasoconstrictor effect of bupivacaine plusepinephrine ; and one on the enucleation of myoma by
morcellation while it is attached to the uterus We did notidentify a randomized controlled trial that assessed the effect of
Our inclusion criteria were randomized controlled trials (RCTs)
uterine artery ligation or laser dissection of the myoma. In 5
that compared the effect of interventions with placebo or no
studies, myomectomy was carried out by laparotomy and in 2
treatment to reduce blood loss during myomectomy. Study
studies it was by laparoscopy. Both laparotomy and
participants were premenopausal women undergoing myomect-
vaginal routes were used in one trial .
Further details about the study participants, interventions,
trials with 58 participants: WMD [random] − 298.72 mL, 95%
type of myomectomy, quality of included studies, and outcomes
CI − 593.10 to − 4.34) (. Though the two trials of
vasopressin showed significant reduction in blood loss,there was significant heterogeneity between them
(P b 0.00001, I2 = 98.7%), presumably due to use of differenttypes of vasopressin: natural vasopressin (1 trial with 20
participants: WMD − 450.00 mL, 95% CI − 507.49 to
− 392.51) and synthetic vasopressin (1 trial with 38
We found no evidence of a difference between oxytocin and
participants: WMD − 149.60, 95% CI − 178.22 to − 120.98).
placebo in blood loss (1 trial with 94 participants: WMD
However, we found no evidence that vasopressin has an
57.00 mL, 95% CI −129.22 to 243.22), need for blood trans-
effect on the need for blood transfusion (1 trial with 20
fusion (OR 1.99, 95% CI 0.88–4.54), and duration of surgery
participants: OR 0.05, 95% CI 0.00–1.03), duration of
(WMD 4.00 min, 95% CI −1.49 to 9.49).
surgery (1 trial with 38 participants: WMD − 28.50 min, 95%CI − 61.76 to 4.76), duration of hospital stay (1 trial with 38
participants: WMD 0.55 days, 95% CI − 0.10 to 1.20), post-operative adhesions to the bowel/omentum (1 trial with 38
Compared to placebo, misoprostol significantly reduced
participants: OR 2.02, 95% CI 0.54–7.49), post-operative
blood loss (1 trial with 25 participants: WMD −149.00 mL,
adnexal adhesions (1 trial with 38 participants: OR 1.87,
95% CI −229.24 to −68.76), shortened duration of surgery
95% CI 0.39–8.93), and occurrence of pregnancy one year
(WMD −9.50 min, 95% CI −15.90 to −3.10) and increased
after myomectomy (1 trial with 38 participants: OR 0.64,
post-operative hemoglobin (WMD 0.80 g/dL, 95% CI 0.33–
1.27). However, there was no evidence of effect on the needfor blood transfusion (OR 0.36, 95% CI 0.05–2.50), duration ofhospital stay (WMD 0.00 days, 95% CI −0.82 to 0.82), and
febrile morbidity (OR 1.25, 95% CI 0.24–6.44).
Compared to placebo, bupivacaine plus epinephrine signifi-
3.3. Vasopressin and analogues of vasopressin
cantly reduced blood loss (1 trial with 60 participants: WMD −
68.60 mL, 95% CI −93.69 to −43.51) and duration of surgery
Compared to participants on placebo, those on vasopressin
(WMD −30.50 min, 95% CI −37.68 to −23.32). No patient
and analogues had a significant reduction in blood loss (2
Characteristics of trials included in the review
15 IU oxytocin IV infusion vs physiological serum Laparotomy Pre-operative blood loss, blood transfusion,
Laparotomy Pre-operative blood loss, operation time,
hospital stay, adhesions and pregnancyoutcome
Laparotomy Post-operative hemoglobin and hematocrit,
for chemical dissection of myoma vs saline for
duration of operation, hospital stay, and post-
400 μg misoprostol vaginally 1 h before surgery Laparotomy Pre-operative blood loss, post-operativevs identical placebo.
hemoglobin, operation time, blood transfusion,hospital stay, and post-operative morbidity.
Laparotomy Pre-operative blood loss and blood transfusion.
vasopressin during surgery vs injection ofplacebo
Enucleation of myoma by morcellation while
Laparoscopy Pre-operative blood loss, hospital stay, and
technique of complete enucleation followed bymorcellation.
Laparotomy Pre-operative blood loss, need for blood
50 mL of bupivacaine cloridrate 0.25% + 0.5 mL Laparoscopy Pre-operative blood loss and operation time. of epinephrine infiltrated into myometriumaround the myoma before incision vsinfiltration of normal saline
A systematic review of randomized controlled trials
Comparison of blood loss (mL): vasopressin and analogues vs placebo or no treatment.
3.5. Mesna (sodium-2-mercaptoethanesulfonate)
the conclusion that blood loss was significantly lower withvasopressin vs placebo is valid. However, more trials are
Chemical dissection with mesna significantly reduced the
needed to quantify the actual estimate of benefit from
duration of surgery (1 trial with 58 participants: WMD
vasopressin. Heterogeneity was thought to be due to the
−20.00 min, 95% CI −28.60 to −11.36) and hospital stay (WMD
differences in blinding of outcome assessors and the fact that
−1.00 day, 95% CI −1.12 to −0.88). Post-operative hemoglobin
one study used natural vasopressin, while the other study
(WMD 0.50 g/dL, 95% CI 0.42–0.58) and hematocrit (WMD
used ornithine vasopressin (ornipressin), a synthetic analo-
1.90 g/dL, 95% CI 1.30–2.50) were also significantly increased
gue of vasopressin in which ornithine is found in position 8 of
with mesna compared to placebo, but there was no evidence of
effect on the incidence of post-operative fever (OR 0.14, 95%
The injection of bupivacaine plus epinephrine into the
myometrium overlying the myoma was evaluated in one studyand the result showed evidence of reduction in blood loss,
although this might not be useful clinically (68.6 mL). Vaso-pressin and bupivacaine plus epinephrine are known localvasoconstrictors and may reduce local blood flow when
Occlusion of the uterine and ovarian arteries signifi-
injected around the myoma. The study on the effect of che-
cantly reduced blood loss (1 trial with 28 participants:
mical dissection of the myoma with mesna did not directly
WMD − 1870.00 mL, 95% CI −2547.16 to −1192.84) and the
evaluate blood loss, but showed a significant gain in post-
need for blood transfusion (OR 0.02, 95% CI 0.00–0.23).
operative hemoglobin. Mesna is a lytic agent that can disrupt
However, the procedure had no evidence of effect on the
connections between tissue layers and may thus
operating time (WMD −4.00 min, 95% CI −29.28 to 21.28).
The largest effect on blood loss during myomectomy was
recorded by the study that combined the occlusion of theuterine arteries and ovarian arteries using tourniquets prior
Myoma enucleation by morcellation during laparoscopic
to myoma enucleation. The uterus receives blood supply
myomectomy reduced the operating time (1 trial with 48
primarily from the uterine artery and secondarily from the
participants: WMD −25.30 min, 95% CI −44.23 to −6.37), but
ovarian artery. Misoprostol, a prostaglandin E2 analogue, was
there was no evidence of effect on blood loss (WMD
equally shown to significantly reduce blood loss, probably by
65.40 mL, 95% CI −36.47 to 167.27) and duration of hospital
causing uterine contraction and reducing uterine blood flow.
stay (WMD −0.07 days, 95% CI −0.18 to 0.04).
Other interventions have not been able to demonstrate
the expected effect on blood loss that was theoretically
postulated. The trial on oxytocin, a known uterotonic agent,showed no evidence of effect on blood loss during myomect-
This review evaluated the effect of different interventions
omy. This is consistent with other evidence that the myo-
on blood loss during myomectomy for uterine fibroids. We
metrial concentration of oxytocin receptors is very low in
identified 8 well designed randomized trials that have
non-pregnant uteri . Similarly, myoma enucleation by
assessed the effect of each intervention on blood loss. All
morcellation showed no evidence of reducing blood loss
during myomectomy. This could partly be due to the small
Some of the interventions showed promising effects on
reducing blood loss during myomectomy. Significant reduc-
One way of evaluating difficulty encountered during
tion of intraoperative blood loss (298.72 mL) was noted when
myomectomy was by measuring operation time. The trials
vasopressin is injected into the uterine muscles overlying the
on misoprostol, bupivacaine plus epinephrine, mesna, and
myoma during myomectomy. Inspection of the data shows
myoma enucleation by morcellation all recorded a signifi-
that the WMD was less than zero in each of the two studies
cant reduction in operation time. The use of oxytocin, peri-
that assessed the effect of vasopressin on blood loss;
cervical tourniquet, and vasopressin showed no evidence of
however, the confidence intervals did not overlap suggesting
highly significant heterogeneity (P b 0.00001, I2 = 98.8%).
Post-operative outcome was assessed by duration of
Thus despite considerable heterogeneity, we believe that
hospitalization. Four trials included the duration of hospital
stay in their evaluation. Only the trial on mesna recorded a
[2] Lethaby A, Vollenhoven B, Sowter M. Pre-operative GnRH
significant decrease in the duration of hospital stay.
analogue therapy before hysterectomy or myomectomy for
There is insufficient data on the adverse effects and costs
uterine fibroids (Cochrane Review). The Cochrane Review, Issue
of different interventions. Trials that commented on adverse
2, 2004. UK: John Wiley & Sons Ltd: Chichester.
[3] Liu W, Tzeng C, Yi-Jen C, Wang P. Combining the uterine
effects simply stated that no adverse effects were noted in
depletion procedure and myomectomy may be useful for
their trial. Knowledge of adverse events and tolerability of an
treating symptomatic fibroids. Fertil Steril 2004;82:205–10.
intervention is important because we have to be able to
[4] Morita M, Asakawa Y, Uchiide I, Nakakuma M, Kubo H. Surgery
balance the estimated benefits, and the harms and costs
results using different uterine wall incision directions in
before making any appropriate decisions about use or non-use
laparoscopic myomectomy of the intramural myoma. Reprod
of the intervention. Evidence from clinical practice has
shown that mesna is well tolerated and can be taken orally
[5] Ngeh N, Belli A, Morgan R, Manyonda I. Pre-myomectomy
uterine embolization minimizes operative blood loss. Br J
In developed countries GnRH analogues have been used
prior to myomectomy. There is now clear evidence that the
[6] Rossetti A, Paccosi M, Sizzi O, Zulli S, Mancuso S, Lanzone A.
Dilute ornitin vasopressin and a myoma drill for laparoscopic
use of GnRH analogues reduces uterine volume and fibroid
myomectomy. J Am Assoc Gynecol Laparosc 1999;6:189–93.
size and may reduce blood loss and operating time during
[7] Higgins JPT, Green S, editors. Cochrane Handbook for Systema-
myomectomy Although the use of pre-operative GnRH
tic Reviews of Interventions 4.2.5 [updated May 2005].
analogues leads to less frequent vertical incisions in the case
of myomectomy, a review of the cost-effectiveness of GnRH
analogues found that the costs outweigh its benefits In
[8] Fletcher H, Frederick J, Hardie M, Simeon D. A randomized
addition, uterine artery embolization (UAE) has been used as
comparison of vasopressin and tourniquet as hemostatic agents
an alternative to myomectomy or to prevent hemor-
during myomectomy. Obstet Gynecol 1996;87:1014–8.
rhage during myomectomy However, there are currently
[9] Ginsburg ES, Benson CB, Garfield JM, Gleason RE, Friedman AJ.
no randomized trials on the effect of UAE on blood loss during
The effect of operative technique and uterine size on blood lossduring myomectomy: a prospective randomized study. Fertil
myomectomy. In low and middle income countries, the cost
of using GnRH analogues and UAE may be prohibitive
[10] Kimura T, Kusui C, Matsumura Y, Ogita K, Isaka S, Nakajima A, et
(especially where there is out-of-pocket payment) and the
al. Effectiveness of hormonal tourniquet by vasopressin during
necessary technology may not be available.
myomectomy through vasopressin V1a receptor ubiquitouslyexpressed in the myometrium. Gynecol Obstet Investig 2002;54:
[11] Sapmaz E, Celik H, Altungil A. Bilateral ascending uterine
artery ligation vs tourniquet use for hemostasis in cesarean
At the moment, there is limited evidence from only a few
myomectomy. A comparison. J Reprod Med 2003;48:950–4.
randomized controlled trials that the use of misoprostol,
[12] Sapmaz E, Celik H. Comparison of the effects of the ligation of
vasopressin, bupivacaine plus epinephrine, pericervical
ascending branches of bilateral arteria uteria with tourniquet
tourniquet, and chemical dissection with mesna may reduce
method on the intra-operative and post-operative hemorrhage
blood loss during myomectomy. However, since we did not
in abdominal myomectomy cases. Eur J Obstet Gynecol Reprod
include trials with head-to-head comparison, we cannot
draw any conclusion about the superiority of one interven-
[13] Assaf A. Adhesions after laparoscopic myomectomy: effect of
the technique used. Gynaecol Endosc 1999;8:225–9.
tion over the other. At present, there is no evidence that
[14] Frederick J, Fletcher H, Simeon D, Mullings A, Hardie M.
oxytocin and myoma enucleation by morcellation have an
Intramyometrial vasopressin as a haemostatic agent during
effect on intraoperative blood loss.
There is need for more well-designed randomized
[15] Celik H, Sapmaz E. Use of a single preoperative dose of
controlled trials to shed more light on the effectiveness of
misoprostol is efficacious for patients who undergo abdominal
different interventions to reduce blood loss during myo-
myomectomy. Fertil Steril 2003;79:1207–10.
mectomy. Apart from the effectiveness, data on the cost-
[16] Agostini A, Ronda I, Franchi F, Bretelle F, Roger V, Cravello L, et al.
effectiveness, pregnancy (if desired) and adverse effects of
Oxytocin during myomectomy: a randomized study. Eur J Obstet
different interventions need to be documented. This is
Gynecol Reprod Biol 2005;118:235–8.
important for clinical decision-making since such decisions
[17] Taylor A, Sharma M, Tsirkas P, Di Spiezio Sardo A, Setchell M,
Magos A. Reducing blood loss at open myomectomy using triple
should be based on the trade off between benefits on the one
tourniquets: a randomized controlled trial. Int J Gynecol Obstet
hand and costs and adverse events on the other.
[18] Benassi L, Lopopolo G, Pazzoni F, Ricci L, Kaihura C, Piazza F, et al.
Chemically assisted dissection of tissues: an interesting support inabdominal myomectomy. J Am Coll Surg 2000;191:65–9.
[19] Zullo F, Palomba S, Corea D, Pellicano M, Russo T, Falbo A, et al.
We wish to thank the Cochrane Collaboration for helping in
Bupivacaine plus epinephrine for laparoscopic myomectomy: a
the development of the protocol and in realization of the
randomized placebo-controlled trial. Obstet Gynecol 2004;104:
[20] Sinha R, Hedge A, Warty N, Mahajan C. Laparoscopic myomect-
omy: enucleation of the myoma by morcellation while attachedto the uterus. J Minim Invasive Gynecol 2005;12:284–9.
[1] LaMote AI, Lalwani S, Diamond MP. Morbidity associated with
[21] Denaro V, Forriol F, Di Martino A, Denaro L, Papalia R, Caione G.
abdominal myomectomy. Obstet Gynecol 1993;82:897–900.
Effect of a mucolytic agent on collagen fibres. An optical and
A systematic review of randomized controlled trials
polarized light histology study. Eur J Orthop Surg Traumatol
[24] Farquhar CM, Brown PM, Furness S. Cost-effectiveness of
preoperative gonadotrophin releasing analogues for women
[22] Fuchs AR, Fuchs F, Husslein P, Soloff MS. Oxytocin receptors in
with uterine fibroids undergoing hysterectomy or myomect-
the human uterus during pregnancy and parturition. Am J
[25] Lumdsden MA. Embolization versus myomectomy versus
[23] Burkert H. Clinical overview of mesna. Cancer Treat Rev 1983;10
hysterectomy: which is best, when? Hum Reprod 2002;17:
The collection of proceedings of Institute Topical problems of NLS diagnostics (theoretical and clinical) CONTENTS: Computer non linear diagnostics . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 5Clinic Tech Inc. — ascending into the XXI century . . . . . . . . . . . . . . . . . 7Method of computer non linear analysis and its role in diagnostics . . . . . 9Pote
CaCu Invasor, Diagnostico, Tratamiento y Seguimiento. Estudio en México. En la actualidad se considera que el cáncer cervico uterino es una de las neoplasias potencialmente curables. La posibilidad de detectar en forma temprana ésta neoplasia hace factible reducir la mortalidad secundaria al padecimiento, sin embargo, este sigue siendo uno de los principales tumores en la mujer, y contribuye c
 International Journal of Gynecology and Obstetrics (2008) 100, 4–9
a v a i l a b l e a t w w w. s c i e n c e d i r e c t . c o m
w w w. e l s e v i e r. c o m / l o c a t e / i j g o
A systematic review of randomized controlled trials toreduce hemorrhage during myomectomy foruterine fibroids ☆
E.J. Kongnyuy a,⁎, N. van den Broek a, C.S. Wiysonge b
a Child and Reproductive Health Group, Liverpool School of Tropical Medicine, Liverpool, UK
b South African Cochrane Centre, South African Medical Research Council, Cape Town, South Africa
Received 8 May 2007; accepted 13 May 2007
Objective: To assess the effectiveness and safety of interventions to reduce blood loss during
myomectomy. Methods: Electronic searches of the Cochrane Library, MEDLINE, and EMBASE,
between 1966 and 2006 for randomized controlled trials (RCTs). Results: We found significant
reductions in blood loss with vaginal misoprostol (weighted mean difference [WMD] −149.00 mL,
95% confidence interval [CI] −229.24 to −68.76); intramyometrial vasopressin and analogues
(WMD −298.72 mL, 95% CI −593.10 to −4.34); intramyometrial bupivacaine plus epinephrine(WMD −68.60 mL, 95% CI −93.69 to −43.51); and pericervical tourniquet (WMD −1870.00 mL, 95%CI −2547.16 to −1192.84). There was no evidence of effect in blood loss with myoma enucleationby morcellation and oxytocin. Conclusion: There is limited evidence from a few RCTs that someinterventions may reduce bleeding during myomectomy. There is need for adequately poweredRCTs to shed more light on the effectiveness, safety, and cost of different interventions to reduceblood loss during myomectomy.
International Journal of Gynecology and Obstetrics (2008) 100, 4–9
a v a i l a b l e a t w w w. s c i e n c e d i r e c t . c o m
w w w. e l s e v i e r. c o m / l o c a t e / i j g o
A systematic review of randomized controlled trials toreduce hemorrhage during myomectomy foruterine fibroids ☆
E.J. Kongnyuy a,⁎, N. van den Broek a, C.S. Wiysonge b
a Child and Reproductive Health Group, Liverpool School of Tropical Medicine, Liverpool, UK
b South African Cochrane Centre, South African Medical Research Council, Cape Town, South Africa
Received 8 May 2007; accepted 13 May 2007
Objective: To assess the effectiveness and safety of interventions to reduce blood loss during
myomectomy. Methods: Electronic searches of the Cochrane Library, MEDLINE, and EMBASE,
between 1966 and 2006 for randomized controlled trials (RCTs). Results: We found significant
reductions in blood loss with vaginal misoprostol (weighted mean difference [WMD] −149.00 mL,
95% confidence interval [CI] −229.24 to −68.76); intramyometrial vasopressin and analogues
(WMD −298.72 mL, 95% CI −593.10 to −4.34); intramyometrial bupivacaine plus epinephrine(WMD −68.60 mL, 95% CI −93.69 to −43.51); and pericervical tourniquet (WMD −1870.00 mL, 95%CI −2547.16 to −1192.84). There was no evidence of effect in blood loss with myoma enucleationby morcellation and oxytocin. Conclusion: There is limited evidence from a few RCTs that someinterventions may reduce bleeding during myomectomy. There is need for adequately poweredRCTs to shed more light on the effectiveness, safety, and cost of different interventions to reduceblood loss during myomectomy.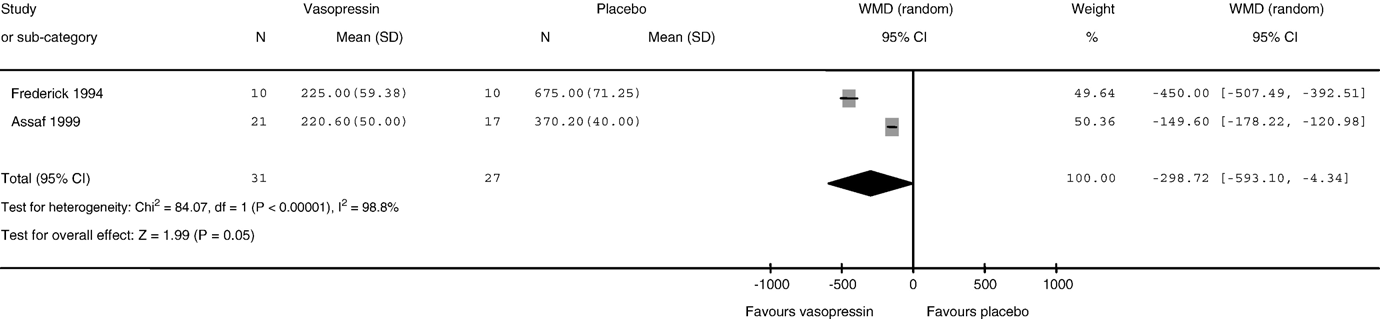 A systematic review of randomized controlled trials
Comparison of blood loss (mL): vasopressin and analogues vs placebo or no treatment.
A systematic review of randomized controlled trials
Comparison of blood loss (mL): vasopressin and analogues vs placebo or no treatment.