Int Urogynecol JDOI 10.1007/s00192-010-1294-y
Long-term results of intravesical hyaluronan therapyin bladder pain syndrome/interstitial cystitis
Paul F. Engelhardt & Nike Morakis & Lukas K. Daha &Britta Esterbauer & Claus R. Riedl
Received: 2 August 2010 / Accepted: 20 September 2010
# The International Urogynecological Association 2010
Introduction and hypothesis While the short-term efficacyof intravesical hyaluronan for bladder pain syndrome/
Glycosaminoglycan (GAG) substitution therapy is one of the
interstitial cystitis (BPS/IC) has been demonstrated, no data
most popular regimens for treatment of BPS/IC. Response rates
exist on the long-term outcome of this therapy.
between 30% and 80% have been described with intravesical
Methods Seventy BPS/IC patients treated with intravesical
administration of various substances like hyaluronan, pentosan
hyaluronan therapy from 2001 to 2003 were asked to rate their
polysulfate (PPS), heparin; chondroitin sulfate, and DMSO.
present status of bladder symptoms on a visual analog scale.
Most of these studies were uncontrolled and short-term
Results Forty-eight of 70 patients responded after a mean
observational. Despite acceptable response rates in these
follow-up of 4.9 years. The average initial VAS score of 8.15
reports, no significant advantage over placebo was found when
had been reduced to 2.71 after therapy and further to 2.14
5 years later. Fifty percent of patients (24/48) reported
One of the largest published series on intravesical hyalur-
complete bladder symptom remission at 5 years follow-up
onan therapy in BPS/IC from our institution showed >80%
without any additional therapy; 41.7% (20/48) with symptom
symptom response rate 6 months after treatment in a therapy-
recurrence was improved with hyaluronan maintenance
naïve group of patients selected by a positive modified
therapy. No improvement was reported by four patients.
potassium test []. Since long-term follow-up data for patients
Conclusions Besides a high rate of acute symptom remis-
after instillation therapy are only addressed in a single study
sion, intravesical hyaluronan also shows long-term efficacy
from Kallestrup for a small patient cohort ], we assessed
in a considerable number of BPS/IC patients.
the present bladder symptom status of our patients 5 yearsafter instillation therapy.
Keywords Bladder pain syndrome . GAG substitution . Hyaluronan . Hyaluronic acid . Instillation therapy . Interstitial cystitis
Seventy female patients with the diagnosis of BPS/IC
P. F. Engelhardt (*) : N. Morakis : C. R. Riedl
Department of Urology, Landesklinikum Thermenregion Baden,
bladder pain syndrome (BPS) is made on the basis of the
symptom of pain related to the urinary bladder, accompa-
nied by at least one other urinary symptom such as day-time and night-time frequency, as well as exclusion of
L. K. DahaDepartment of Urology, Krankenhaus Hietzing,
confusable diseases as the cause of the symptoms”) who
had been treated with intravesical hyaluronan 40 mg in50 cm3 phosphate-buffered saline (Cystistat®, Bioniche,
Urologic Clinic, Paracelsus University of Medicine,
with a questionnaire by mail. Patients were selected for
hyaluronan therapy by a positive modified potassium test, i.
symptoms recurred during the first year after initial
e., patients had to show a >30% reduction of maximal
improvement in 20/48 patients (41.7%). These recurrences
bladder capacity in a consecutive instillation of saline
were treated with another course of weekly hyaluronan
(NaCl 0.9%) and KCl 0.2 M as described by Daha et al.
instillations followed by monthly maintenance therapy in
These patients received weekly hyaluronan instilla-
12 patients, supported by a daily dose of oral pentosanpo-
tions until symptoms resolved as to patients judgement or if
lysulfate in another eight patients. The VAS at present
instillation therapy turned out to be ineffective after a
follow-up for this group with maintenance treatment was
maximum of 10 instillations. Instillation therapy was only
2.4. The four nonresponders were also treated with a
performed in patients who were able to retain the
combination of intravesical hyaluronan and oral PPS to
maximize GAG substitution therapy, and later with
The questionnaire was identical to questionnaires before
alternative therapies like amitryptilin, however, without
and after instillation therapy as published before and asked
VAS scores before therapy and throughout follow-up
are shown in Tables and as well as Fig. . The
1. The present status of global bladder symptoms (“Please
average initial VAS score for all patients was 8.15 (SD ±
rate the presently perceived intensity of your bladder
1.67), decreased to 2.71 (SD ± 1.96) immediately after
symptoms”) by a visual analog scale (VAS, 0 to 10,
hyaluronan therapy, stayed stable at 6 months post
where 0 is no symptoms and 10 is intolerable bladder
instillation therapy with an average 2.7 (SD ± 2.1), and
showed a further reduction to 2.14 (SD ± 2.31) 5 years
2. Additional therapies within the last 5 years
later. VAS score reduction after therapy was statistically
3. And a global judgement of instillation therapy (“Would
you undergo instillation therapy again?” and “Would
A VAS score reduction of >2 was observed in 85.4% of
you recommend instillation therapy to other patients?”)
patients (41/48), whereas 6.25% (3/48) showed a reduction
Improvement was defined as a VAS score reduction of
<2%, and 8.3% (4/48) reported no improvement. While
initial VAS scores were similar for three treatment groups
Statistical analysis was performed by Friedman ANOVA
(group 1: single course of intravesical hyaluronan with
and Kendall Coefficient of Concordance Test (p<0.05) and
permanent remission, group 2: repeat course and mainte-
nance of hyaluronan therapy, group 3: maintenance withintravesical hyaluronan and oral PPS), group 1 had thelowest VAS score after 5 years of follow-up (1.4) vs. 2.4 in
group 2 and 4.1 in group 3 that included the fournonresponders.
The response rate to the questionnaire was 68.5% (48 of 70
No statistical correlation was found between patient age
patients). Patients’ demographics are shown in Table
or duration of BPS/IC symptoms and the grade of symptom
Average patients’ age was 48.3 years (17–81), and the
average time period after the last instillation was 4.9 years(4–6.8). The average duration of bladder symptoms in thispatients group had been 6.1 years (0.5–12 years) before
initiation of treatment. The average number of instillationswas 11.8 (8–25).
The efficacy of hyaluronan is based on several mechanisms
Table shows the long-term outcome of hyaluronan
that aim on the urothelial function disorder present in BPS/IC:
instillation therapy: 50% of patients (24/48) were free of
on one side, hyaluronan reinforces the urine-tissue barrier by
bladder symptoms after hyaluronan instillation therapy for
integration in the GAG layer on the luminal surface and the
the whole observation period; their VAS was 1.4 at present
base of urothelial cells; on the other side, unique antiin-
follow-up. While only 8.3% (4/48) of patients did not
flammatory mechanisms have been identified, like inhibition
experience any benefit from hyaluronan therapy, bladder
of leukocyte migration, adherence of immune complexes, and
Mean disease duration before hyaluronan therapy
Total numbers of hyaluronan instillations mean
Table 2 Long-term follow-up after initial hyaluronan instillation therapy
Stable symptom improvement after primary therapy without any further therapy during follow up
Stable symptom improvement with intermittent hyaluronan instillation therapy during follow up
Stable symptom improvement with intermittent hyaluronan instillation therapy and oral PPS during follow up
binding to specific receptors (I-CAM 1, CD 44) involved in
treated with intravesical hyaluronan for 3 months (four
weekly and two monthly instillations) and were followed
The present report is the first that assesses treatment
for 3 years. After the initial 3 months of treatment, 65% of
results 5 years after hyaluronan instillation therapy. Even
patients reported symptom improvement (nocturia was
with the setback of an uncontrolled study and a nonre-
reduced 40%, pain 30%) and continued monthly hyalur-
sponse rate to the questionnaire of 31.5% which reduces the
onan instillations up to 3 years. About 50% of these
response rate in an intention-to-treat analysis to 34%, there
patients stopped therapy within this 3 years period because
are several important conclusions that can be drawn from
of complete symptom remission, while the other 50% still
kept monthly maintenance therapy and were judged aspartial responders. These data are confirmed by the present
1. Intravesical hyaluronan therapy may lead to persistent
symptom remission in a selected group of BPS/IC
Similar results as in the present study have not been
patients. In conventional terms, these patients, 50% in
reported for other GAG substituents. Response rates after
the present survey, may be regarded as cured from their
initial instillation therapy were 45% for chondroitin sulfate,
disease. However, late recurrences surpassing the
56% for heparin, and 44% for PPS Long-term results
observation period cannot be excluded.
2. Part of the patients with symptom remission after
The high response rate in the present study may be a
intravesical hyaluronan therapy relapses early within
consequence of patient selection and standardization of
the first year; however, treatment response was main-
tained by continuation of instillation therapy through-out the whole observation period. In some patients, oral
1. The modified potassium test is believed to indicate a
PPS was added to the GAG substitution regimen, if
disorder at the urine-tissue barrier. Only patients with a
either they were not able to regularly come to
positive test were included in the present study. This set
instillations for an extended period of time or if
of patient responds better to GAG substitution therapy,
hyaluronan therapy alone did not improve symptoms
whereas potassium negative patients show a very low
response rate of about 20% –Only recently, it
3. Hyaluronan long-term therapy has no adverse effects
was shown that successful hyaluronan instillation
and can be administered over years without disadvan-
therapy with symptom remission reverses positive
The only comparable long-term results were reported by
2. Patients were treatment-naive for BPS/IC, i.e. hyaluronan
Kallestrup in this series, 20 BPS/IC patients had been
therapy was their first disease-specific therapy. Patients
VAS reduction 5 years after initial hyaluronan therapy
VAS 1–2 (mild symptoms, no subjective need for therapy)
VAS >2 (moderate symptoms, request for therapy)
Table 4 VAS scores in responders, maintenance therapy and non-responder groups
Group 1 (CR after HA) Group 2 (HA maintenance) Group 3 (PPS+HA maintenance) responders non-responders
CR complete remission, Ha hyualuronian, PPS pentosan polysulfate
with a number of unsuccessful preceding treatments
which counteract the beneficial effect of intravesical
represent a negative selection of possibly advanced or
neuropathic disease, which usually does not respond to
5. The 8.3% of patients that did not respond to hyaluronan
instillation therapy stayed unimproved after 5 years, i.e.
3. The average number of instillations was almost 12 in
also other therapies that were initiated during this
the present series and, thus, appreciably higher than in
period did not influence symptomatology. This subset
the reports of other investigators that normally used a
of BPS/IC patients stays the “hard core” that needs to
schedule of four weekly followed by two to four
be subject of future investigations.
4. To be eligible for the protocol, patients had to be able
In summary, besides a high rate of acute symptom
to retain the hyaluronan instillation for at least 2 h.
remission, intravesical hyaluronan also showed long-term
Shorter bladder contact times show less efficacy. Thus,
efficacy in a considerable number of BPS/IC patients in the
patients with low bladder capacities (and possibly more
present study, which suggests that some patients may be
advanced disease) were not included. Anti-infective
cured by this therapy. Patients with symptom recurrence
prophylaxis with nitrofurantoin 50 mg on instillation
after instillation therapy have a high chance for symptom
days prevented bladder infections from catheterism,
remission with hyaluronan maintenance therapy.
Fig. 1 Box plot figure of VASsymptom score during follow-up
Claus R. Riedl is the principal investigator for
9. Riedl CR, Engelhardt PF, Daha KL, Morakis N, Pflüger H (2008)
controlled study on Hyaluronan in BPS/IC (CISTIC).
Hyaluronan treatment of interstitial cystitis/painful bladder syn-drome. Int Urogyneocol J Pelvic Floor Dysfunct 19(5):717–721
10. Kallestrup EB, Steinunn S, Jørgense S, Nordling J, Hald T (2005)
Treatment of interstitial cystitis with Cystistat®: a hyaluronic acid
product. Scand J Urol Nephrol 39:143–147
11. Daha LK, Riedl CR, Hohlbrugger G, Knoll M, Engelhardt PF, Pfluger
1. Toft BR, Nordling J (2006) Recent developments of intravesical
H (2003) Comparative assessment of maximal bladder capacity, 0.9%
therapy of painful bladder syndrome/interstitial cystitis: a review.
NaCL versus 0.2M KCl, for the diagnosis of interstitial cystitis: a
prospective controlled study. J Urol 170:807–809
2. Morales A, Emerson L, Nickel JC, Lundie M (1996) Intravesical
12. Hurst RE (1994) Structure, function, and pathology of proteoglycans
hyaluronic acid in the treatment of refractory interstitial cystitis. J
and glycosaminoglycans in the urinary tract. World J Urol 12:3–10
13. Leppilahti M, Hellström P, Tammela TLJ (2002) Effect of
3. Fall M, Oberpenning F, Peeker R (2008) Treatment of bladder
diagnostic hydrodistension and four intravesical Hyaluronan
pain syndrome/interstitial cystitis 2008: can we make evidence-
Instillations on bladder ICAM-1 intensity and association of
ICAM-1 intensity with clinical response in patients with intersti-
4. Porru D, Campus G, Tudino D, Valdes E, Vespa A, Scarpa RM,
Usai E (1997) Results of treatment of refractory interstitial cystitis
14. Schulz A, Vestweber AM, Dressler D (2009) Anti-inflammatory
with intravesical hyaluronic acid. Urol Int 59:26–29
action of a hyaluronic acid-chondroitin sulphate preparation in an
5. Bade JJ, Laseur M, Nieuwenburg A, van der Weele LT,
in vitro bladder model. Akt Urol 40(2):109–112
Mensink HJ (1997) A placebo controlled study of intravesical
15. Parsons CL, Forrest J, CJ CJ, the Elmiron Study Group (2002)
pentosanpolysulfate for the treatment of interstitial cystitis. Br J
Effect of pentosan polysulfate therapy on intravesical potassium
6. Parsons CL, Housley T, Schmidt JD, Lebow D (1994) Treatment of
16. Gupta SK, Pidcock L, Parr NJ (2005) The potassium sensitivity test:
interstitial cystitis with intravesical heparin. Br J Urol 73:504–507
a predictor of treatment response in interstitial cystitis. BJU Int
7. Steinhoff G, Ittah B, Rowan S (2002) The efficacy of
chondroitin sulfate 0.2% in treating interstitial cystitis. Can J
17. Teichman JM, Nielsen-Omeis BJ (1999) Potassium leak test
predicts outcome in interstitial cystitis. J Urol 161:1791–1796
8. Nickel JC, Egerdie B, Downey J, Singh R, Skehan A, Carr L, Irvine-
18. Daha L, Riedl CR, Lazar D, Simak R, Pflüger H (2008) Effect of
Bird K (2009) A real-life multicentre clinical practice study to
intravesical glycosaminoglycan substitution therapy on bladder
evaluate the efficacy and safety of intravesical chondroitin sulphate
pain syndrome/interstitial cystitis, bladder capacity and potassium
for the treatment of interstitial cystitis. BJU Int 103(1):56–60
sensitivity. Scand J Urol 42(4):369–372
SERVICES VETERINAIRES AMBULATOIRE EQUIN EQUINE AMBULATORY VETERINARY SERVICES Dre Alix Serapiglia Rappel: choses à faire-penser avant accouplement / insémination Examen reproducteur de la jument et examen physique general Durée de gestation: 335-345 jours en moyenne Règle générale, les juments gestantes sont traitées de la même façon que les autres chevaux jusqu’à envir
http://www.medscape.com/viewarticle/807694_printEye Therapy Has It Over Antidepressant for PTSDDeborah BrauserEDINBURGH, Scotland — Eye movement desensitization and reprocessing (EMDR) may be a more efficacious treatment for patientswith posttraumatic stress disorder (PTSD) than antidepressant medication, new research suggests. A smal , randomized trial of male survivors of the ongoing war in
 Int Urogynecol JDOI 10.1007/s00192-010-1294-y
Long-term results of intravesical hyaluronan therapyin bladder pain syndrome/interstitial cystitis
Paul F. Engelhardt & Nike Morakis & Lukas K. Daha &Britta Esterbauer & Claus R. Riedl
Received: 2 August 2010 / Accepted: 20 September 2010
# The International Urogynecological Association 2010
Introduction and hypothesis While the short-term efficacyof intravesical hyaluronan for bladder pain syndrome/
Glycosaminoglycan (GAG) substitution therapy is one of the
interstitial cystitis (BPS/IC) has been demonstrated, no data
most popular regimens for treatment of BPS/IC. Response rates
exist on the long-term outcome of this therapy.
Int Urogynecol JDOI 10.1007/s00192-010-1294-y
Long-term results of intravesical hyaluronan therapyin bladder pain syndrome/interstitial cystitis
Paul F. Engelhardt & Nike Morakis & Lukas K. Daha &Britta Esterbauer & Claus R. Riedl
Received: 2 August 2010 / Accepted: 20 September 2010
# The International Urogynecological Association 2010
Introduction and hypothesis While the short-term efficacyof intravesical hyaluronan for bladder pain syndrome/
Glycosaminoglycan (GAG) substitution therapy is one of the
interstitial cystitis (BPS/IC) has been demonstrated, no data
most popular regimens for treatment of BPS/IC. Response rates
exist on the long-term outcome of this therapy.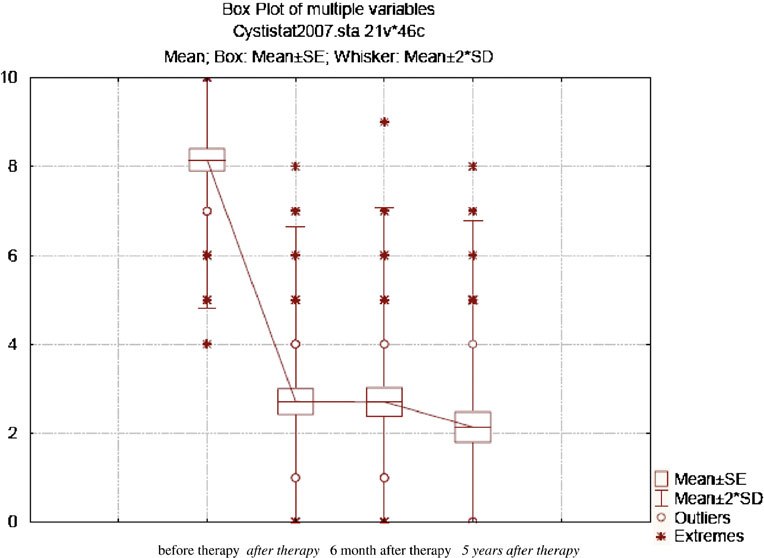 Table 4 VAS scores in responders, maintenance therapy and non-responder groups
Group 1 (CR after HA) Group 2 (HA maintenance) Group 3 (PPS+HA maintenance) responders non-responders
CR complete remission, Ha hyualuronian, PPS pentosan polysulfate
with a number of unsuccessful preceding treatments
which counteract the beneficial effect of intravesical
represent a negative selection of possibly advanced or
neuropathic disease, which usually does not respond to
5. The 8.3% of patients that did not respond to hyaluronan
instillation therapy stayed unimproved after 5 years, i.e.
Table 4 VAS scores in responders, maintenance therapy and non-responder groups
Group 1 (CR after HA) Group 2 (HA maintenance) Group 3 (PPS+HA maintenance) responders non-responders
CR complete remission, Ha hyualuronian, PPS pentosan polysulfate
with a number of unsuccessful preceding treatments
which counteract the beneficial effect of intravesical
represent a negative selection of possibly advanced or
neuropathic disease, which usually does not respond to
5. The 8.3% of patients that did not respond to hyaluronan
instillation therapy stayed unimproved after 5 years, i.e.